Most SSDI cases do not fail because the claimant isn’t disabled.
They fail because the evidence is unusable.
That is the uncomfortable operational truth of the SSD system.
Behind every denial that says “insufficient evidence” is not a lack of medical care, but a file full of fragmented records, missing timelines, generic notes, and zero functional clarity. The system does not reward effort, honesty, or personal testimony. It rewards documentation that fits how SSA actually evaluates disability.
And most SSD teams are losing at that layer.
How Medical Records Are Used in SSDI Decisions
There is a dangerous assumption baked into most SSD workflows:
“If we collect enough medical records, the truth will speak for itself.”
It won’t.
Raw records are chaotic by default. They are written for billing, not adjudication. They are scattered across providers, inconsistent in structure, and almost never focused on functional limitations. A 2,000-page file with no narrative is not strong evidence. It is noise.
From an SSA perspective, more pages do not equal more proof.
Only structured, functional, decision-ready evidence matters.
What “Accurate” Actually Means in SSDI
In SSDI, accuracy is not about volume. It is about alignment.
Records must match the claimed conditions, cover the relevant time period, show consistent treatment, include objective findings, and (most critically) translate medical data into functional limitations.
SSA is not deciding whether someone is sick.
They are deciding whether someone can work.
If the file cannot answer basic functional questions, the outcome is already leaning toward denial, regardless of how real the condition is in everyday life.
Common Problems With SSD Medical Records
The single most common failure point LMS sees across SSD operations is functional blindness.
Files confirm diagnoses but never explain:
- How long someone can sit or stand
- How often do symptoms interfere
- How medications affect capacity
- What mental or cognitive limits exist
Without this layer, DDS and ALJs are forced to fill in the gaps themselves, often through consultative exams and third-party opinions.
Once that happens, control of the case leaves the treating evidence and moves into the hands of external evaluators who have never seen the claimant before.
From the LMS’s perspective, these are not rare edge cases. They are systemic problems that appear in a large percentage of SSD files.
How Poor Records Affect the SSD Workflow
Most SSD teams treat medical summaries as a nice-to-have. In reality, they are the only way complex medical data becomes usable inside SSA.
A real summary does not paraphrase records. It extracts:
- timelines
- patterns
- severity
- functional limits
- evidentiary relevance
This is the layer where most SSD workflows either succeed or quietly collapse.
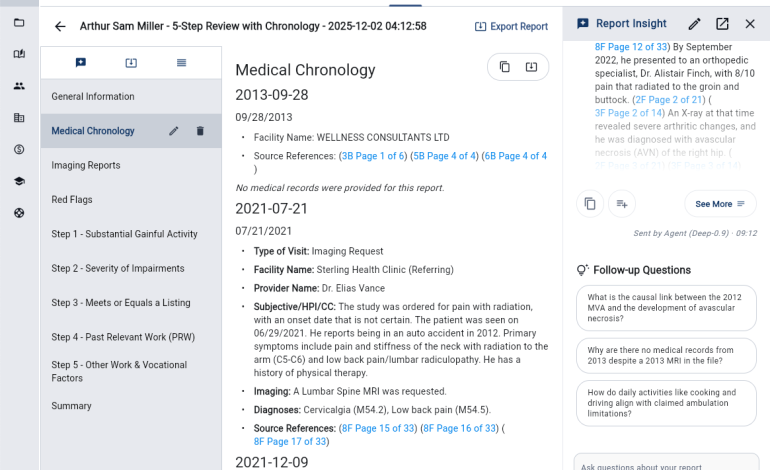
The Role of Medical Summaries in SSD Cases
Because SSD files often contain thousands of pages of raw records, medical summaries play a critical operational role. A proper summary organizes medical data, identifies relevant providers and timelines, highlights key diagnoses, extracts functional limitations, and creates a clear narrative.
This is where LMS makes a difference. Our summaries translate fragmented documentation into structured, decision-ready evidence that aligns with how SSA evaluates claims. Summaries do not replace original records, but they make it possible for decision-makers to actually understand them, turning chaos into operational control and dramatically increasing the odds of a favorable outcome.
The LMS Point of View
LMS exists because the SSD system is structurally broken at the evidence layer.
We see the same pattern across case volumes:
- bloated files
- missing function
- delayed development
- CE dependency
- decisions based on gaps, not reality
Our work is not about collecting more records. It is about making records operational.
Structured medical review, functional extraction, and decision-ready summaries are not enhancements. They are the difference between a file that can be evaluated and one that quietly fails.
Why Accuracy Directly Impacts Outcomes
SSDI is not decided by stories, sincerity, or perceived severity. It is decided by whether the evidence fits the machine. Most SSD teams feed that machine raw, unstructured data and hope for the best. That is not a strategy. That is wishful thinking disguised as process.
If your SSD cases rely on massive record dumps, inconsistent summaries, or third-party exams to fill evidentiary gaps, LMS provides structured medical review and summary systems designed specifically for how SSA actually makes decisions.